The Price You Cannot See
Pediatric pay is capped not by the value of the work but by the price of the payer — and where the system patches that gap, it routes the correction through channels the physician is never shown.
I. Two bills for the same morning
The two children came through on the same morning, an hour apart. The visits were, for any purpose a clinician would recognize, identical: the same length, the same examination, the same shortness of breath worked up the same way, the same spirometry, the same conversation with a worried parent about the same inhaler. The notes, read side by side, differ only in the names.
The remittances, when they arrive weeks later, do not match. One pays meaningfully more than the other. Nothing in the medicine accounts for the difference. The child who generated the smaller payment was not seen for less time, did not receive less care, and did not present a less complicated problem. The only variable that moved between the two encounters was the payer — and behind the payer, a fact about the child that has nothing to do with the work: which program insures them.
Every pediatrician learns to stop noticing this, the way you stop hearing a sound that is always there. But it is worth holding onto the strangeness of it for a moment, because the entire architecture of pediatric compensation is built on top of it. The work was priced, and then the price was overruled by something about the patient. The question this essay asks is what that something is, and — by the end — why, in the place most pediatric subspecialists actually work, they are not permitted to see it at all.
II. The work was never the variable
The mechanics are not in dispute, and they are not hidden. They are published.
Medicare pays physicians off a single national schedule. Each service carries relative value units — for the physician work, the practice expense, the malpractice cost — set the same way everywhere in the country, adjusted for local cost, and multiplied by one nationally fixed conversion factor that turns relative value into dollars. A given service has, in effect, one Medicare price, reached by one transparent formula.
Medicaid does not work this way. Each state sets its own physician fee schedule. As the Medicaid and CHIP Payment and Access Commission (MACPAC) describes it, states may peg their rates to the Medicare relative-value framework, to a flat percentage of the Medicare fee, or to a schedule of their own construction — and “the amount Medicaid pays typically is less than 100 percent of the Medicare amount.” There is no federally prescribed Medicaid physician rate. There are fifty-some of them.
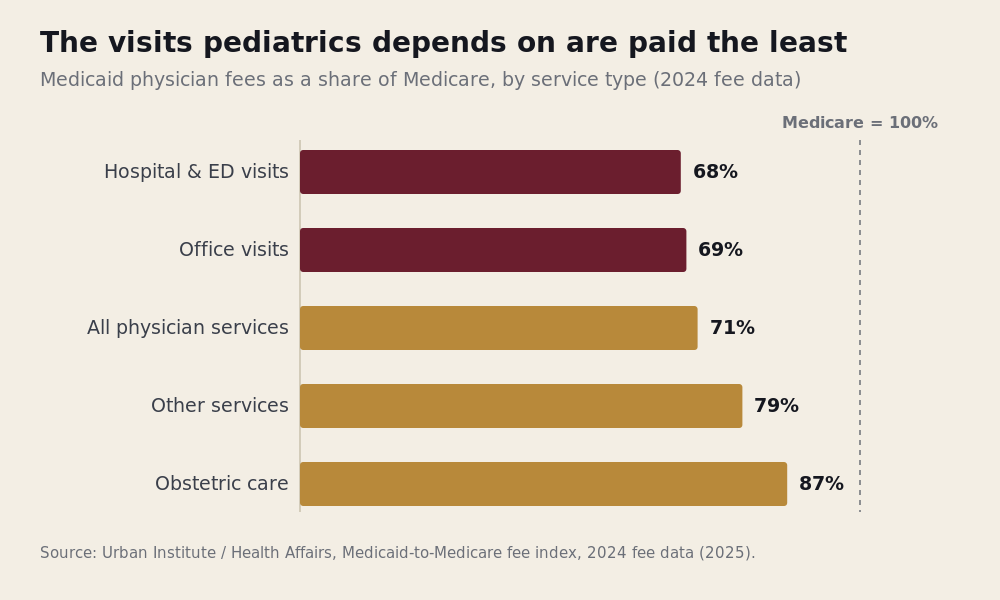
So the same service — the same procedure code, resting on the same relative value units — is run through different multipliers depending on who is paying. The gap is measurable, and it has been measured for decades. The most recent national accounting, published in Health Affairs in 2025 using 2024 fee data, puts Medicaid physician fees at roughly 71 to 75 cents on the Medicare dollar, depending on the basket of services weighed — and lower than that for the office and outpatient visits that make up the bulk of pediatric practice, closer to 68 to 69 percent. MACPAC notes the ratio has been “largely unchanged” since 2008. This is not a transient underpayment working its way out of the system. It is the steady state.
None of this would matter much to pediatrics if children were distributed across payers the way adults are. They are not. Medicaid and CHIP together cover something close to two in five American children by survey measures, and nearly half — about 49 percent — by the administrative enrollment counts the American Academy of Pediatrics analyzed in late 2024. The program that pays physicians the least is the program that insures the most children.
The work, in other words, was never the variable. The payer was. And for children, the payer is fixed against them.
III. Two programs, two constituencies
It is tempting to treat the gap as a budgetary accident — the kind of thing that could be true or false, high or low, by some neutral calculation of what care costs. It is more honest to treat it as a fact about political design.
Medicare and Medicaid were enacted in the same month of 1965, and almost everything about how they pay physicians has diverged since. Medicare is federal, uniform, and updated on a published schedule; its constituency is older Americans, who are numerous, organized, and vote, and whose program has acquired over sixty years the political armor that follows from that. Medicaid is a federal-state partnership administered fifty different ways, means-tested, and perennially in tension with state budgets that must balance every year; its constituency is poor families and their children, who are none of those things.
The consequence shows up most clearly not in the national average but in its spread. The same national figure that reads as “Medicaid pays about three-quarters of Medicare” dissolves, at the state level, into something far wider: in the lowest-paying states the Medicaid physician fee runs at roughly a third of Medicare, while a few states meet or exceed parity, with the state-by-state index varying by a factor of nearly three from bottom to top. A child’s physician is paid for the identical service at radically different rates depending only on which state line the family lives inside. The variation is not clinical. It tracks no difference in what children need. It tracks what each legislature was willing to appropriate.
This is the part of the diagnosis that is easy to state and easy to leave as a grievance: children inherited the weaker program, and the price of their care reflects the political weight of the people who depend on it. True as far as it goes. But it stops one step short of the more interesting fact — which is that the states do not actually believe their own base rates. They spend a great deal of money and ingenuity quietly working around them.
IV. The patches: a system that knows
If the published Medicaid rate were the system’s honest judgment of what pediatric care is worth, you would expect the system to stand behind it. It does not. It patches it — continuously, expensively, and in a way that gives the whole game away. Almost every patch is benchmarked, explicitly, to Medicare. The number the system insists is the market rate for children is the number it keeps straining to escape.
The most direct patches are enhanced fee schedules. Florida is a clean example because it documents itself. Through its Practitioner fee schedule, the state added a 7.3 percent pediatric increase for physicians serving children from birth to age twenty, directed by the legislature in the annual budget. Through a separate managed-care mechanism, the MMA Physician Incentive Program, it lifts qualifying physicians treating children to roughly 106 percent of Medicare — slightly above the adult benchmark — a figure the state’s own analysis reports as 105.6 percent, then 106.2, then 106.3 across three recent rate years. The enhancement is not confined to primary care: pediatric subspecialists — a pulmonologist, a cardiologist, a surgeon — qualify on the same terms as a general pediatrician, for any service rendered to a child under twenty-one. Florida is not unusual in kind, only in clarity; a 2025 multistate review found Virginia paying as much as 191 percent of Medicare for physicians at freestanding children’s hospitals, California moving toward parity through a 2024 ballot measure, and a scatter of other states layering similar increases on top of their base schedules.
Two things about these enhancements matter more than their size. The first is that they are set year to year, through the appropriations process, at the discretion of the legislature and the governor — Florida’s own agency notes that the increases must recur annually just to keep pace as Medicare itself moves. Parity that must be re-voted every spring is not a price; it is a grant that happens to be denominated in the language of a fee. The second is who is eligible for the visible version of it — but that is the subject of the section this essay turns on, and we will come to it.
Beyond the fee schedules, the patches multiply. States run Title V programs for children with special health care needs — in Florida, the Children’s Medical Services program, authorized in its own chapter of state law — which fund care coordination and services that ordinary Medicaid does not reach, and which, through safety-net arms, can extend even to children of families above the Medicaid income line when a condition is serious enough. Teaching hospitals draw graduate medical education payments; because freestanding children’s hospitals see almost no Medicare patients, they are largely shut out of Medicare’s GME funding and so receive a dedicated federal program, Children’s Hospitals GME, built specifically to fill the hole their pediatric payer mix leaves. Medicaid itself paid teaching institutions on the order of $7.4 billion in GME in 2022. Beneath these sit further layers — 340B drug discounting for the hospitals that serve the most Medicaid children, cost-based reimbursement floors for community health centers — each a structural acknowledgment that the base rate does not, on its own, sustain the care.
Where those institutional dollars come from — the provider taxes, the supplemental-payment financing, the federal match that states engineer to draw them down — is a large enough subject, and a contested enough one, to be its own essay; it is the one this series takes up next. For now the narrower point is sufficient: a base rate that requires this much patching is a base rate the system has already judged to be inadequate. The patches are not generosity. They are a confession, entered in the language of appropriations.
And the clearest confession of all came when the federal government, briefly, turned the dial all the way up — and then turned it off.
V. A dial, not a fact
For two years, 2013 and 2014, the Affordable Care Act required every state to raise Medicaid payment for primary care services to 100 percent of Medicare, with the federal government covering the full cost of the increase. For twenty-four months, the asymmetry this essay describes simply vanished for a defined set of services. Then, on schedule, the requirement expired. Congress did not renew it. According to the Urban Institute’s accounting, nineteen states chose to continue the higher rates with their own funds; the rest let them fall back.
This was, in effect, a national experiment in whether the Medicaid price is a fixed fact or an adjustable choice — and it answered the question twice. When the rates went up, access followed: a study in the New England Journal of Medicine using audit callers across ten states found the share of primary care offices offering a new Medicaid patient an appointment rose from 58.7 to 66.4 percent over the period of the increase, with the largest gains where the raises were largest, and with no lengthening of wait times. When the rates later fell, a follow-up found the gains partly reversed. The evidence is not unanimous — MACPAC characterizes the access research as mixed — but the direction is hard to miss. The number moved, and the world moved with it.
A price that can be raised by a federal vote, sustained by a state legislature, and dropped by an expiration date is not the verdict of a market discovering what pediatric work is worth. It is a policy lever wearing the costume of a fee. And it is a lever any reader can locate without taking anyone’s word for it. Find your state’s Medicaid-to-Medicare fee index — it is published — or take a single common pediatric code and put its Medicare allowed amount beside what your state’s Medicaid pays for it. The exercise costs a few minutes and returns a single, blunt number: the discount your state has decided a child’s care will carry this year. It will not be the same as the number a neighboring state decided. That, by itself, is the proof.
Which raises the question that the patches were quietly building toward all along. When the dial is turned up — when the system does pay pediatric care at parity, or above it — who actually gets to see that it happened?
VI. The price you can see, and the price you can’t
Here the structure splits in two, and the split is the most important fact in this essay.
For a physician in private practice, the correction is visible and it is theirs. The enhancement that lifts pediatric pay toward — and past — parity flows to the practitioner who did the work; the rate is published, the physician bills against it, and whatever margin it produces stays with the practice. The number can be looked up, contested, planned around. It is a price in the ordinary sense — something a person can see and act on.
For a physician inside an institution, the same correction arrives, but it arrives somewhere they cannot look. Florida’s headline enhancement — the managed-care program that lifts qualifying physicians to 106 percent of Medicare — explicitly excludes “Medical School Faculty Plans,” and it does so, in the state’s own words, “regardless of whether or not the service is billed by the Medical School Faculty Plan as a plan service or by the rendering provider using their own Medicaid ID.” What disqualifies the academic physician is not their specialty — the identical pediatric pulmonologist or cardiologist in private practice qualifies for the same enhancement as any general pediatrician — but the channel their work is billed through. The academic pediatrician does not receive the visible raise. Their parity — and for many institutions it reaches or exceeds parity — comes instead through channels that never resolve into a per-service rate: supplemental payments that MACPAC notes states make to physicians “typically those employed by state university hospitals,” disproportionate-share and upper-payment-limit dollars computed in the aggregate for the institution, graduate medical education funds that state law carves out of physician payment entirely and routes to the teaching hospital. The money is real and it is often larger than what private practice receives. But it is delivered as institutional block payments, routed through institutional leadership, and the physician who generated the underlying care will never see the effective rate for their own services.
Set this beside the first essay in this series, and the loop closes. The compensation benchmarks a physician negotiates against are produced by the buy side of the labor market; the salary an institution offers is set against those benchmarks; and the actual revenue the physician’s work commands — which, after all the patches, may meaningfully exceed what the salary implies — is held one level up, in an aggregate the physician is not shown. It becomes structurally possible for a physician to be paid less than the work brings in and to have no way, from inside, to know it.
It would be dishonest to present this only as extraction, because the institutional model does something private practice cannot. Cross-subsidy is what allows an unprofitable subspecialty to exist at all. A pediatric pulmonologist, a geneticist, a metabolic specialist serving a small and heavily Medicaid population may generate professional fees that no independent practice could survive on; folded into an institution that pools the GME, the facility revenue, the supplemental payments, and the inpatient margin, that same physician becomes viable, and the children get a specialist who would otherwise not be in the region. Under honest governance, the opacity is simply the back office of a system doing something genuinely hard and genuinely good.
The cost is what opacity does to a person. A physician who cannot see the value of their own work is not merely underinformed; they are placed in a position where the value can be told to them. When the institution controls both the number and the narrative about the number, the ordinary frictions of employment acquire a particular shape — the persistent, unfalsifiable suggestion that one is fortunate to be carried, that the work does not quite cover its cost, that the doubt one feels about one’s own worth is a private failing rather than the predictable product of being denied the figure that would settle it. The gaslighting that physicians describe, and the impostor’s doubt so common it is treated as a personality trait, are not always psychological in origin. Sometimes they are what it feels like to stand inside an information asymmetry that was built for other reasons and happens to fall on you.
This is also, finally, why the map of pediatric practice looks the way it does — subspecialty care almost entirely inside academic centers, primary care surviving outside in some states and not others. It is not a mystery and it is not only a matter of call schedules. Subspecialty care lives where the opaque cross-subsidies live, because only there does the arithmetic close. Primary care, paid closer to the visible fee, lives or dies by that fee — which is why its independent practice thrives in the parity states and thins out in the ones that pay a third of Medicare. The compensation structure did not just set the prices. It chose, payer by payer and patch by patch, who would get to be their own boss.
VII. What an honest accounting would separate
There is a genuinely hopeful reading available here, and it should be said plainly rather than buried. Where a state has patched the visible fee to parity, the economics of independent pediatric primary care are far better than the headline Medicaid rate suggests — good enough, in a parity state, to make hanging a shingle in an underserved, Medicaid-heavy county a defensible decision rather than a charitable one. The opportunity is real. It is simply rationed by geography and granted at the legislature’s annual discretion, and it is largest in exactly the visible channel that the institutional model is structured to bypass.
An honest compensation conversation would not require abolishing any of this. It would require separating two things the current system fuses: the value of the work and the price of the payer. It would make the second visible to the person performing the first. A physician inside an institution would be able to see the effective rate their services actually command — not as a courtesy, but as the precondition for any of the words we use about fair pay to mean anything at all. You cannot negotiate against a number you are not allowed to see. You cannot even know whether you are being treated well.
So the portable question at the end of this one is not the market’s question but its inverse. Not what is the rate for this work — the rate, it turns out, was never the hard part. The harder question, the one the structure is built to keep you from asking: for the work you did this morning, what was actually paid for it — and who decided that you would never find out?
Satyanarayan Hegde, MD, is a pediatric pulmonologist and the founder of Access Pediatric.