The Scarcity That Doesn't Pay
In every other market, scarcity raises the price. In physician subspecialty labor it lowers it — and the reason is not a paradox but a name economists already have for it.
I. The rarer doctor, paid less
There are more pediatric cardiologists in the United States than pediatric nephrologists, and the cardiologist is paid more. State it that way and nothing seems wrong; cardiology simply sounds like the bigger, better-compensated field. But turn the sentence around to face what it actually says, and the strangeness surfaces. The scarcer specialty — the one a family must drive farther to reach, the one missing from more of the country’s hospital referral regions — is the one that pays less. The rarer the doctor, the smaller the lifetime reward for becoming one.
I am a pediatric pulmonologist. By the standard measures I am rarer than a pediatric cardiologist and rarer still than a general pediatrician, and by those same measures I will earn less across a career than either. For a long time I read that as a fact about my field — a quirk of where the procedures are, what insurance pays for a breathing test, which subspecialties happen to sit where on the income ladder. It is only when the whole distribution is laid out at once that the quirk resolves into a pattern, and the pattern into something closer to a law.
The law is this: in the market for subspecialty physician labor, scarcity does not raise the price. It tracks the opposite direction. And the reason is not that the laws of supply and demand have been suspended for medicine. It is that the market this labor is sold into is not the market most physicians think they are in.
II. What scarcity is supposed to do
Begin with the thing everyone already knows, because the whole argument turns on how completely it fails to hold here. When a good is scarce relative to demand, its price rises. That is not a sophisticated claim; it is the first diagram in the first week of the first economics course, and it governs almost everything a physician buys — the house near the good school district, the seat on the oversold flight, the rare-earth metal in the scanner. Scarcity is leverage. The scarce party names a higher number, and the market pays it because the alternative is going without.
Medicine half-believes this about itself. The phrase “physician shortage” is spoken as though it were also a forecast of rising pay: if doctors are scarce, surely the scarce ones will be bid up. The trade press reinforces it, the recruitment campaigns assume it, the premed imagines it. The intuition is so automatic that its failure, when you finally look at the data, reads as an error in the data rather than a fact about the world.
The data does not read that way to the economist who assembled it. In 2021, Eva Catenaccio and colleagues published, in Pediatrics, a calculation of the lifetime financial return to each pediatric subspecialty fellowship measured against the alternative of practicing as a general pediatrician. The headline result was already sobering: the returns “ranged from +$852 129 for cardiology to −$1 594 366 for adolescent medicine,” and “twelve of 15 subspecialties analyzed yielded negative financial returns.” Most pediatric subspecialties, in other words, cost a physician money over a career relative to not subspecializing at all. The training is longer, the entry into earning is delayed, and the salary at the end does not repay the gap.
But the finding that matters for this article is the companion one, published the same year in JAMA Pediatrics, where Catenaccio’s team set lifetime earning potential beside the geography of the workforce itself. The scarcer the subspecialty, the lower its pay — and they measured scarcity three separate ways and got the same answer each time.
III. The inversion, measured three ways
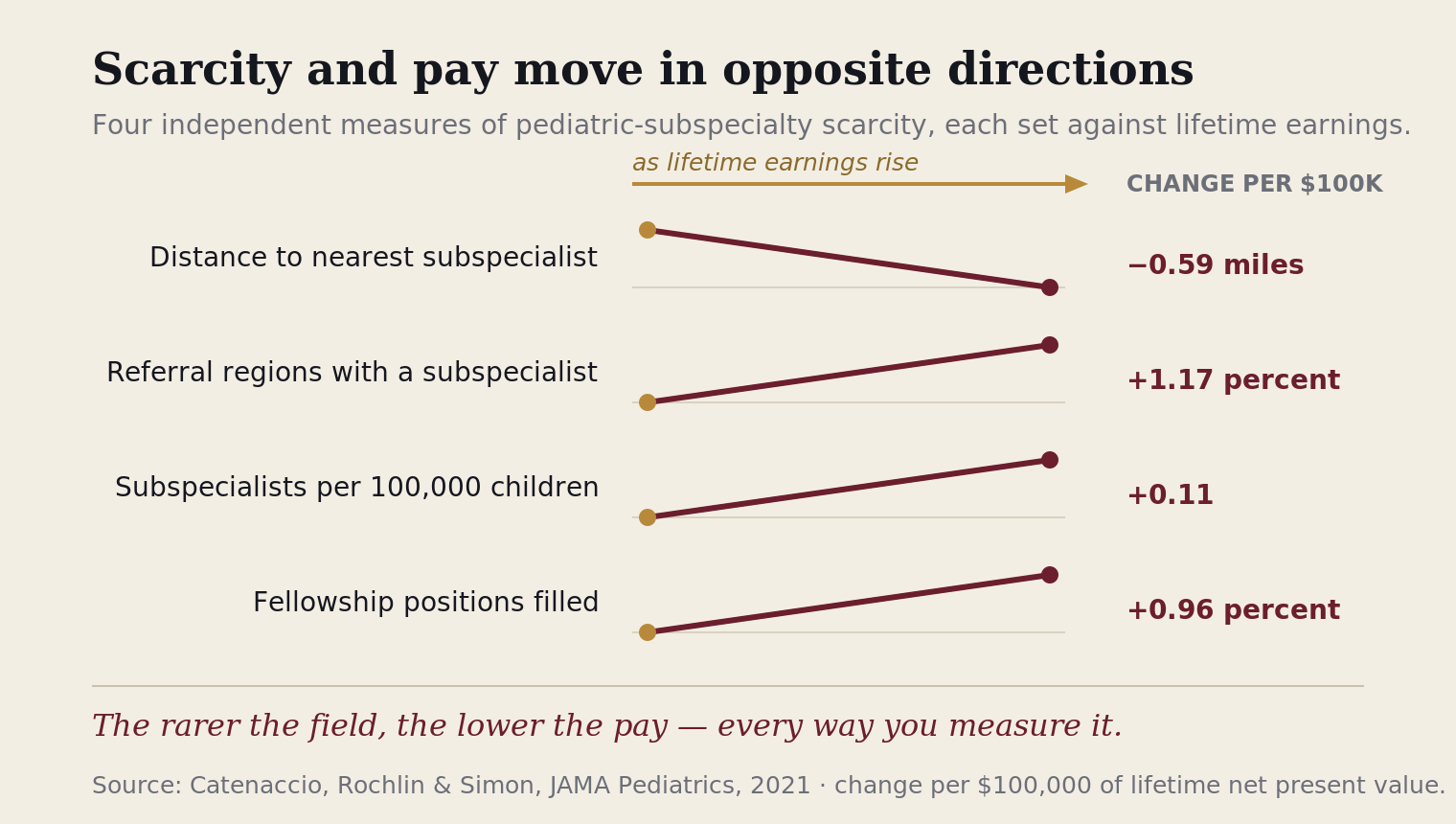
Scarcity is a slippery thing to quantify, so the JAMA Pediatrics analysis used three independent proxies for it and regressed each against lifetime net present value. The first was distance: how far, on average, a family must travel to reach a subspecialist in that field. The second was coverage: the share of the country’s hospital referral regions that have at least one certified subspecialist of that type. The third was density: the number of subspecialists per 100,000 children.
In a market where scarcity raised price, all three would slope the way scarcity is supposed to — the rarer fields paying more to compensate for the rarity. Every one of them sloped the other way. Higher lifetime NPV was associated with a shorter average distance to care, with presence in more referral regions, and with higher per-capita density. The better-paid the subspecialty, the more of it the country had. The worse-paid, the scarcer. Pay and abundance moved together; pay and scarcity moved apart.
The fellowship pipeline closes the loop. The same analysis found that a higher lifetime NPV predicted a higher fellowship fill rate, and put a number on the indifference point: a lifetime NPV of about $5.48 million was the level at which a subspecialty would fill all its training slots. Above it, fields overfilled; below it, they went wanting. Cardiology, with the highest lifetime NPV in the study at roughly $6.45 million, filled 106 percent of its positions. Nephrology, near the bottom at about $4.29 million, filled 65 percent. The market is not failing to send a signal. It is sending a perfectly clear one, and trainees are reading it correctly: the scarce fields are scarce because they pay less, and they will stay scarce as long as they do.
This is the point at which the pattern stops looking like a feature of pediatrics and starts looking like a feature of the market structure. Nothing in the biology of nephrology makes it less valuable than cardiology to a sick child; the child whose kidneys are failing needs the nephrologist as urgently as the child in heart failure needs the cardiologist, and the nephrologist is harder to find. A market that rewarded value to the patient, or scarcity of the provider, would pay the nephrologist more. This one pays less. The question is what kind of market does that.
IV. The name for it
There is a name for it, and it is not new. A market with many sellers and one buyer — or a few buyers acting at arm’s length from one another — is a monopsony, the mirror image of monopoly. In a monopoly the single seller sets the price above what competition would yield. In a monopsony the single buyer sets it below. The classic illustration in every labor textbook is the company town: when one mill is the only employer for fifty miles, the mill does not have to match anyone’s wage, because there is no one to match. The worker’s options are the mill or the road out of town, and the mill knows it.
What monopsony does to scarcity is the crucial part, because it is exactly counter to intuition. In a competitive labor market, a scarce skill commands a premium — the few who have it are bid over by the many who want it. In a monopsonized one, scarcity can do the reverse. When the sellers of a skill are few and scattered and cannot coordinate, and the buyers are concentrated and patient, fewness becomes a weakness rather than a lever. A subspecialty with two hundred practitioners nationwide has no bargaining bloc, no comparator down the street, no second bidder across town. Each of the two hundred negotiates alone, against an institution that employs many and will still be there when the one walks away. The very rarity that should have been leverage instead means there is no thick market to set a competing price.
The cleanest direct evidence that buyer concentration suppresses medical wages comes, for now, from the workers adjacent to physicians rather than physicians themselves. In a 2021 paper in the American Economic Review, Elena Prager and Matt Schmitt studied what happened to wages after hospital mergers that meaningfully increased local employer concentration. For workers whose skills were specific to the industry — the people who could not simply carry their training to a non-hospital employer down the road — wage growth slowed measurably after the largest mergers, by roughly four percent for skilled workers and nearly seven percent for nurses and pharmacy workers over the following years, relative to where wages would otherwise have gone. Mergers that did not increase local concentration produced no such effect. The mechanism was not malice. It was structure: fewer buyers, skills that do not travel, and the wage that follows.
Physicians sit squarely inside that structure, and more so every year. By the Physicians Advocacy Institute’s accounting, 77.6 percent of U.S. physicians were employed by hospitals, health systems, or other corporate entities as of January 2024, up from less than half a decade earlier. A pediatric subspecialist is among the most concentrated cases of all: subspecialty care is overwhelmingly hospital-based and academic, which means that in many metropolitan areas the number of plausible employers for a given subspecialty can be counted on one hand, and in many regions it is one. The skills are maximally industry-specific — there is no off-ramp for a pediatric pulmonologist’s training outside of pediatric pulmonology — and the buyers are maximally concentrated. That is the company town, rendered in subspecialty medicine. The law scholars Suresh Naidu, Eric Posner, and Glen Weyl argued in the Harvard Law Review that labor monopsony is both widespread and under-policed; subspecialty physician labor may be one of its purest specimens.
I want to be precise about the strength of this claim, because the discipline of this journal is to mark the line between what is documented and what is inferred. That hospital consolidation directly lowers physician pay is, as of now, an inference — the clean causal studies are for nurses and pharmacists, and the pediatric pattern is consistent with monopsony rather than proof of it. What is documented is the structure: the inverse relationship between scarcity and pay, the concentration of buyers, the immobility of the skill. Monopsony is the name that fits the structure. It is not the only force in the room, and the next section gives the competing account its due.
V. The honest competing account
The mainstream explanation for low pediatric subspecialty pay is not monopsony. It is reimbursement, and it deserves a fair hearing because it is substantially true.
Pediatrics is the most public-payer-dependent field in medicine, and Medicaid pays well below Medicare for the same work. A subspecialty whose patients are disproportionately children, disproportionately Medicaid-covered, and disproportionately treated through cognitive rather than procedural care collects less revenue per hour than an adult, commercially insured, procedure-heavy counterpart — and compensation, eventually, follows revenue. The National Academies’ consensus report on the pediatric subspecialty workforce locates the problem there, in the payment schedule and the procedural mix, not in the structure of the labor market. This journal has made the same argument at length about the field as a whole, in The Shortage That Isn’t: the pediatric problem is largely a payer problem wearing a headcount costume.
Catenaccio’s own papers are scrupulous about the limits of a purely financial model. The authors note that their calculation “cannot capture the many other factors beyond economic concerns” — among them lifestyle, research interest, and the pull of a particular disease — and point out that gastroenterology fills well despite a modest financial return, plausibly because it offers well-reimbursed procedures without the heaviest call burden. These are real forces. A field can be underpaid relative to its scarcity and still attract people who want the work, and the reimbursement schedule can depress a salary without any single buyer lifting a finger.
The reimbursement account and the monopsony account are not rivals; they are layers. Reimbursement sets the size of the pie — the total revenue a subspecialty’s work generates. Monopsony governs the division of it — how much of that revenue reaches the physician versus how much is retained by the institution that employs her. A field can be squeezed on both: paid little because its payer mix is poor, and paid less than even that mix would support because the physician negotiates alone against the only buyer in the region. The reimbursement story explains why the pie is small. It does not, by itself, explain why the scarcest providers — the ones with the least competition for their services and the greatest distance to the nearest substitute — capture the smallest slice. For that, the structure of the buy side has to enter the account.
VI. The recruitment that scarcity does not explain
Here is a test any physician can run against their own experience, and it costs nothing but the willingness to notice.
If a subspecialty is genuinely scarce — if a region has one pediatric nephrologist where it needs three — then the institution trying to hire one is the desperate party. Scarcity should make the buyer move quickly, compete openly, and close fast, because every facially qualified candidate is precious and a rival hospital might take the one who is available. That is how a buyer behaves when the thing it is buying is truly rare and truly needed.
Now set that prediction beside the recruitment process as physicians actually live it. The scarcer the specialty, often, the longer and more elaborate the courtship: the prescreen, the phone interview with a division director, the full day of sequential interviews, the second visit, the committee, the weeks of silence between steps, the offer that arrives only after the candidate has been thoroughly, patiently vetted. A process optimized for a desperate buyer would look nothing like this. A process optimized to establish, over months, that the jobs are scarcer than the doctors — that it is the candidate who must qualify for the position rather than the position that must compete for the candidate — looks exactly like this.
I am describing a pattern, not asserting a motive, and the distinction is the journal’s standing rule. I cannot show that any institution designs its hiring to manufacture an impression of job scarcity; I can only observe that the elaborateness of the process runs opposite to what genuine scarcity of the candidate would produce, and invite the reader to weigh their own experience against the two predictions. When you next sit through the months-long version of this, the question worth holding is simply: if my specialty is so scarce, why is this institution behaving as though the scarce thing in the room is the job, and not me?
There is a second move in the same structure, and this journal has already documented it, so I will not re-argue it here: the numbers a physician negotiates against are themselves produced by the buy side, aggregated from the institutions’ own records and returned to those institutions as “the market.” The Numbers Pediatricians Negotiate Against traces that loop in full. The relevant point for this article is only that it compounds the monopsony. A scarce seller, negotiating alone against a concentrated buyer, is handed — as the definition of fair — a figure assembled by the buyer’s own trade associations. Scarcity confers no leverage; the data confers none either; and the elaborateness of the process quietly establishes that the leverage runs the other way.
None of this is unique to pediatrics. The pediatric subspecialist is the extreme case — the rarest skill, the most concentrated buyer, the poorest payer mix, the clearest inversion — which is exactly what makes the field the right place to see the mechanism without distortion. But every employed physician sits somewhere on the same curve. The adult subspecialist in a consolidated market, the hospitalist whose only local employers are two systems that will not bid against each other, the academic whose compensation is set by a survey her own department reports into — each is a milder reading of the instrument the pediatric subspecialist reads at full scale. The question the rare doctor is forced to ask is the question available to all of them.
It is not what is my specialty worth? The honest version is harder, and it points at the structure rather than the schedule:
If my scarcity is real, who captured the value of it — and why was it not me?
Satyanarayan Hegde, MD, is a pediatric pulmonologist and the founder of Access Pediatric.